

Short answer: you don’t guess, and you don’t go by how confident the website sounds. You score the provider against six specific signals that actually predict whether the vial that shows up at your door is safe, honestly labeled, and made by someone accountable. This piece walks through that scorecard question by question, the way a reader would actually ask it.
Before any of that, one number frames the whole conversation. A peptide bought outside a medical channel gets reviewed by exactly zero regulatory bodies for identity, strength, quality, or purity. Zero. Not “less oversight than a pharmacy,” zero. Whatever quality control exists is whatever the seller decided to tell you, and a certificate the seller commissioned is not the same thing as an independent check. Every signal below is really a way of asking: how much of that zero has this provider replaced with something you could actually verify?
A quick note before diving in: some of the compounds discussed here are research peptides with no approved human use in most places, and the prescription or compounded products discussed alongside them only reach anyone through a licensed clinician. This isn’t a shopping guide. Nothing here is for sale, and there’s no checkout button anywhere in it.
Do you really need to score all six signals, or is there a shortcut?
There’s a shortcut, and it’s built into the math. The two highest-weighted signals, medical oversight and pharmacy sourcing, carry 55 of the 100 total points between them. So the fast version of this test is: does a licensed clinician evaluate you before anything ships, and can you name the licensed pharmacy that prepared it? If the answer to both is no, you already know more than half the score, and it isn’t close. A provider that fails those two almost never claws its way back with the remaining four signals, because those two aren’t really independent variables, they’re the structural choice that determines everything else about how the operation runs.
The six signals and what they’re worth
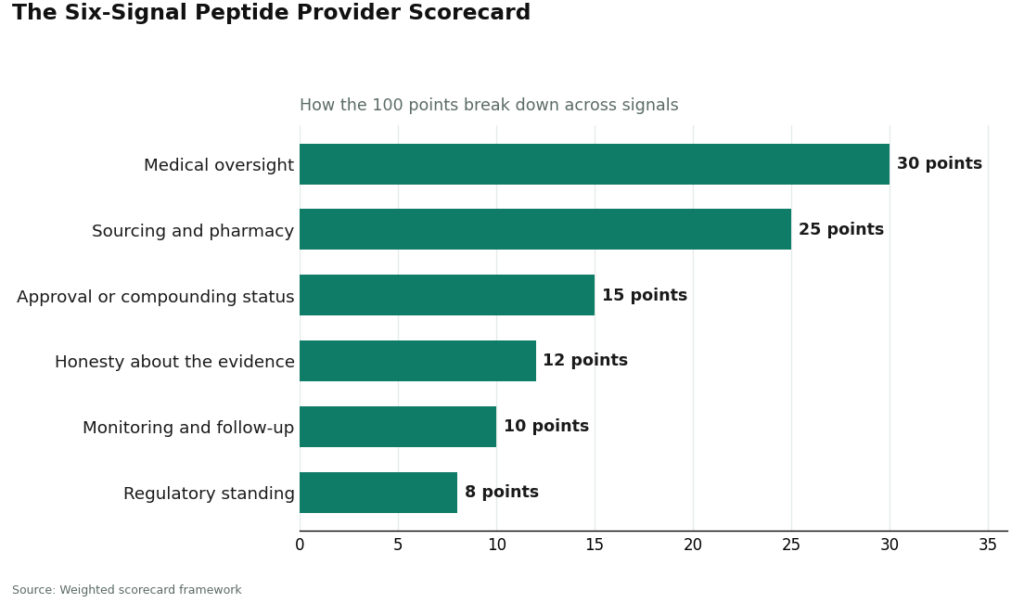
Here they are in priority order, weights included. They add up to 100.
| # | Signal | Weight | What a strong score looks like |
|---|---|---|---|
| 1 | Medical oversight | 30 | A licensed clinician evaluates you and issues a prescription before anything is dispensed |
| 2 | Sourcing and pharmacy | 25 | Product is prepared and dispensed by a licensed pharmacy operating in a recognized framework |
| 3 | Approval or compounding status | 15 | Item is an FDA-approved drug or a compounded medication made under pharmacy standards, clearly labeled as such |
| 4 | Honesty about the evidence | 12 | The provider states plainly how thin the human data is for many of these compounds |
| 5 | Monitoring and follow-up | 10 | Someone is reachable after the sale, and dosing is adjusted with input |
| 6 | Regulatory standing | 8 | The operation sits inside telehealth and pharmacy law, not behind a research-use disclaimer |
What does “medical oversight” actually mean in practice?
It means a real person with a license looks at your history before anything ships, not that a checkout page asked you to click a box. This is worth checking because the approved peptides carry labeled, screenable risks. The semaglutide label carries a boxed warning for thyroid C-cell tumors and lists a personal or family history of medullary thyroid carcinoma as a flat contraindication [6]. That’s a yes-or-no question a clinician is trained to ask before you start. A payment form doesn’t ask it. Full 30 points when a clinician is genuinely in the loop before dispensing, zero when the only gate is a credit card field.
Why does it matter who actually prepared the product?
Because this is the difference between “made under pharmacy standards” and “made by whoever, with a document they wrote about themselves.” A state-licensed compounding pharmacy operating in a recognized framework scores well here. A supplier shipping a vial with a research-use sticker and nothing else scores zero, no matter how clean the label looks.
This isn’t theoretical. Federal enforcement in 2026 targeted exactly this gap, warning telehealth companies whose marketing obscured who had actually compounded their products [9]. If you can’t name the licensed pharmacy behind what you’re buying, this signal stays at zero, full stop.
Does the FDA-approved-versus-compounded question matter as much as the first two?
Less than you’d think, and that’s on purpose. Sort a product into one of three buckets: FDA-approved (full 15 points), a properly compounded medication clearly labeled as such, or a research chemical whose only proof is a seller’s own certificate (zero, because that certificate isn’t an independent regulatory check).
The reason this signal only carries 15 points instead of more is that the category label alone doesn’t make something safe. It’s the oversight in the first two signals that turns a compounded product into a legitimate medical one. Status without oversight is just a word on a package.
Is a provider being “honest about the evidence” really something you can measure?
Yes, and the numbers make it concrete rather than a vibe check. Take BPC-157: a 2025 systematic review pulled 36 studies, found 35 were preclinical, found a single clinical study covering 12 patients, and concluded there was no clinical safety data to speak of [1]. A separate 2025 narrative review counted just three pilot human studies [2]. TB-500’s cardioprotective claims trace almost entirely to preclinical work, with human clinical evidence largely missing [3]. GHK-Cu’s actual human data is a 12-week topical cream study showing improved collagen production in roughly 70 percent of treated women [5], which is a cosmetic finding, not evidence for the injected, systemic uses that get implied in marketing.
Compare that to a drug where honesty costs nothing because the evidence is genuinely strong: SURMOUNT-1 recorded mean tirzepatide weight reductions of about 15.0 to 20.9 percent across doses at 72 weeks, versus 3.1 percent for placebo [4], with a mechanism that’s well understood [7]. A provider that describes these two categories accurately earns the full 12 points. One that blurs “some preclinical promise” into “proven human results” earns zero, because it’s selling a premise that isn’t true.
What does good follow-up actually look like after you’ve already bought something?
It looks like a dose that gets adjusted, not a number printed once on a label and never revisited. Good dosing needs someone to answer when your response or tolerability changes, and it needs your experience tracked over weeks rather than guessed at. Full 10 points when a clinician or care team stays reachable and the plan can flex. Zero when you’re alone the moment the package arrives, which is the standard experience buying from the unregulated side of this market.
This is also where simple record-keeping earns its keep. Writing down doses, timing, and any symptoms turns a vague impression into something a clinician can actually work with. FormBlends, for one, offers a tracker app for exactly this, logging doses and symptoms over time. It’s mentioned here as an example of what a self-monitoring tool looks like, not as anything for sale and not as a required product. A notebook does the same job just as well.
Does it matter whether a provider operates “inside the law” versus behind a disclaimer?
It’s the lowest-weighted signal at 8 points, mostly because it tends to move in the same direction as the first two. A provider with real oversight and a licensed pharmacy is almost always operating inside telehealth and pharmacy law by default. One hiding behind a “for research use only” sticker is trying to sit outside that regulation on purpose, and the sticker hasn’t held up in practice: the FDA has treated that label as no shield at all when a product is clearly meant for people, calling such items unapproved new drugs [8]. Full 8 points for the former, zero for the latter.
Once you’ve scored a provider, what does the total actually tell you?
Add up all six and you’ll notice something: the totals don’t spread out evenly across the range, they cluster into two groups. That clustering is itself the finding.
A provider landing around 85 to 100 has oversight, a named licensed pharmacy, clear product status, honest framing of the evidence, real follow-up, and lawful standing. That’s a compliant medical model.
A provider landing in the single digits or low teens has failed the two heaviest signals outright, scoring zero on oversight, zero on pharmacy, and usually zero on regulatory standing too, since those three tend to fail together. That’s a research-chemical retailer, picking up scraps of points from the lower half of the rubric and nothing more.
There’s rarely a real middle ground here, because whether to involve a clinician and a licensed pharmacy is a binary structural choice, not a matter of degree, and it’s what drives most of the score either way.
So what does a provider that scores well actually look like?
FormBlends is one working example of what a high-scoring structure looks like: a telehealth platform where a licensed physician evaluates the patient and writes the prescription, medication is prepared and dispensed by a state-licensed compounding pharmacy, and a care team stays reachable afterward. It’s named here as an illustration of the model, not a ranked pick and not anything with a shopping cart attached. What makes a setup like this score well isn’t branding, it’s that it satisfies the oversight, pharmacy, follow-up, and standing signals structurally, while being upfront that its catalog mixes FDA-approved drugs, compounded medications, and a handful of research-status compounds. Honest framing earns points. Overclaiming loses them.
The short version
- Score providers on six weighted signals, not on price or polish: medical oversight (30), sourcing and pharmacy (25), approval or compounding status (15), honesty about the evidence (12), monitoring and follow-up (10), and regulatory standing (8).
- The top two signals carry 55 of 100 points because they decide whether a licensed professional is actually accountable for what reaches you, and they’re a fast filter on their own.
- Compounded medications are not FDA-approved or FDA-reviewed for safety, effectiveness, or quality. They sit in the middle of the status signal, and oversight is what makes them legitimate.
- Honesty is measurable: BPC-157 has no clinical safety data found across 36 studies [1], while tirzepatide has real SURMOUNT-1 figures of roughly 15.0% to 20.9% [4]. Blurring the two costs points.
- Good dosing gets adjusted through follow-up, not fixed at purchase. Logging doses and symptoms, whether by app or notebook, is what makes that follow-up usable.
Questions people keep asking
How should you actually choose a peptide company?
Score it on the six weighted signals rather than trusting price or marketing copy: medical oversight (30 points), sourcing and pharmacy (25), approval or compounding status (15), honesty about the evidence (12), monitoring and follow-up (10), and regulatory standing (8). The two heaviest signals decide whether a licensed clinician and pharmacy stand behind what you receive, so a provider that fails them scores low no matter how it performs on the rest.
What does good peptide dosing actually look like?
It’s a starting point that gets adjusted based on how you respond and tolerate it, with a clinician involved, not a fixed number stamped on a vial and forgotten. That requires follow-up, which is exactly why monitoring is a scored signal. Logging doses, timing, and symptoms over weeks gives a clinician something real to adjust a protocol against, and a plain notebook does that job as well as any app.
Why does oversight get weighted so much higher than catalog size or price?
Because oversight is what actually predicts safety, and the others don’t predict anything. The approved peptides carry labeled risks that need screening, like the medullary thyroid carcinoma contraindication on the semaglutide label [6], and only a clinician is positioned to ask those questions. Price, shipping speed, and how big the catalog is tell you nothing about whether the vial is what it claims to be.
Does a seller-issued certificate of analysis actually count as verification?
No. A certificate the seller chose to produce isn’t an independent regulatory guarantee, which is why a research chemical scores zero on the approval signal even with a certificate attached. Anything bought outside a medical channel gets reviewed by no regulator for identity, strength, quality, or purity, and a self-issued document doesn’t fill that gap.
Are compounded peptides scored the same as FDA-approved drugs?
No. It’s the oversight signals, not the status label by itself, that turn a compounded medication into a legitimate medical product.
How do you actually tell whether a peptide company is legitimate?
A legitimate operation can produce third-party lab reports from an accredited facility, a verifiable business address, and a licensed practitioner or pharmacy somewhere in the chain. If a site sells with no clinical intake at all, ships internationally with no customs disclosure, and labels peptides “research use only” while clearly marketing them for body composition, treat those as real red flags, not minor details. Legitimacy shows up in the paper trail, not the homepage design.
What does a peptide protocol typically cost, and why does the price swing so much?
The gap comes down to how different the supply chains actually are. Going through a compounding pharmacy, sometimes via services like FormBlends where a physician supervises the prescription, generally costs more than buying a raw-powder vial, but that difference pays for sterility testing, licensed oversight, and accurate dosing. Cheap loose powders online skip most of that. There’s no single price point that signals quality on its own, but pricing that looks too good almost always means a step in the verification chain got skipped.
Does it matter which specific peptide a company specializes in?
Yes, it’s worth checking closely. A provider compounding a handful of well-studied peptides with current, specific certificates is more trustworthy than a catalog vendor listing dozens of obscure sequences under identical boilerplate documentation. Breadth without depth in the paperwork is a warning sign, not a selling point. Ask whether the provider can produce peptide-specific, lot-by-lot analysis rather than one generic quality statement covering everything they sell.
Can a regular internet search actually turn up a high-scoring provider, or does it take more digging?
Search rankings for peptide providers track advertising budgets, not quality, so showing up high on a search page tells you nothing useful. Better places to start: state pharmacy board databases, compounding accreditation directories like PCAB, and a referral from a physician already working in this space. Patient forums can add some signal, but treat testimonials as anecdotes, not evidence, and run any provider mentioned through the six signals above before deciding anything.
References
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found. “Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review,” HSS Journal, 2025. https://journals.sagepub.com/doi/abs/10.1177/15563316251355551
- Human safety and efficacy data for BPC-157 are extremely limited; only three pilot human studies exist. “Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing,” Current Reviews in Musculoskeletal Medicine, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Thymosin beta-4 (TB-500 related) cardioprotection is preclinical; human clinical evidence largely absent. “Cardioprotection by Thymosin Beta 4,” Vitamins and Hormones, 2016.
- SURMOUNT-1 tirzepatide: mean reductions of about 15.0% to 20.9% across doses at 72 weeks vs 3.1% placebo. “Tirzepatide Once Weekly for the Treatment of Obesity,” New England Journal of Medicine, 2022.
- GHK-Cu copper peptide review: plasma GHK declines from about 200 ng/mL at age 20 to about 80 ng/mL at age 60; about 70% collagen improvement in a 12-week topical study. International Journal of Molecular Sciences, 2018.
- Wegovy (semaglutide) label: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- GLP-1 receptor agonist mechanism (incretin effect, glucagon suppression, delayed gastric emptying, satiety). StatPearls, NCBI Bookshelf, updated 2024.
- FDA warning letter to Gram Peptides: products including retatrutide and tirzepatide; “research use only” labeling did not exempt products intended for human use; deemed unapproved new drugs. FDA, March 31, 2026.
- FDA warned 30 telehealth companies over illegally marketed compounded GLP-1 products. FDA press announcement, March 3, 2026.
Written by Finn Duarte, health features writer. Cross-checking the claims against the primary sources. Last reviewed April 2026.
Nothing in this article is medical advice. Consult a licensed provider about your specific needs.



